Gender Based Violence in Sudan
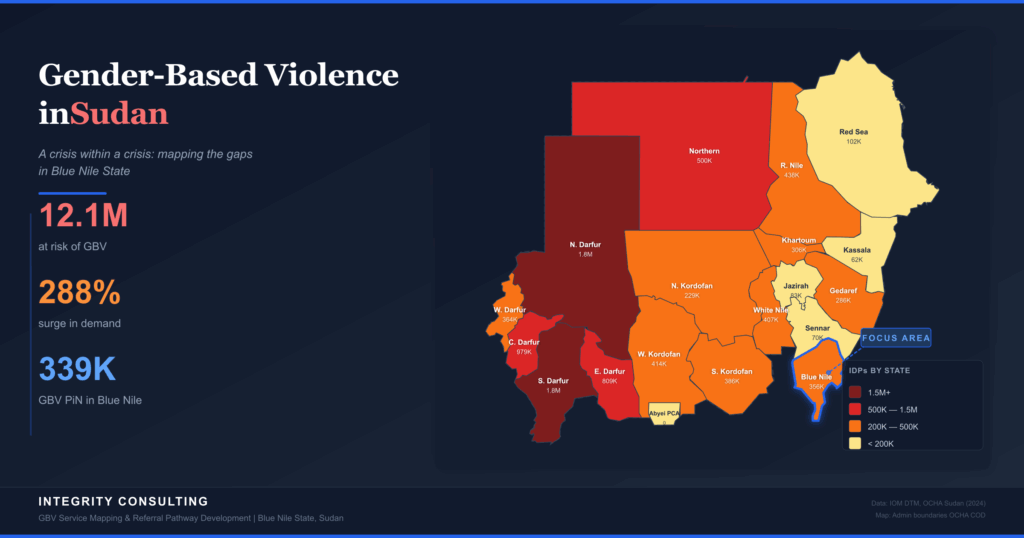
With 12.1 million people at risk and a 288 percent surge in demand for services, Sudan faces the world’s largest gender-based violence crisis — and in Blue Nile State, where service mapping efforts are now underway, two localities have zero GBV actors
Since April 2023, Sudan has been engulfed in an armed conflict between the Sudanese Armed Forces (SAF) and the Rapid Support Forces (RSF) that has produced the world’s largest displacement crisis. Over 12.8 million people have been forced from their homes, 30.4 million — 64 percent of the population — need humanitarian assistance, and amid this catastrophe, gender-based violence has emerged as one of the most devastating yet least addressed dimensions of the crisis.
An estimated 12.1 million people are now at risk of GBV, with demand for services surging by 288 percent in 2025 alone. Sexual violence is being used systematically as a weapon of war. Women and girls, who make up 54 percent of displaced populations, face compounding threats at every stage of displacement — in conflict zones, along flight routes, and within overcrowded camps and host communities.
The Unfolding Crisis
What began as a power struggle between two military factions in Khartoum has rapidly metastasised into a nationwide conflict affecting all 18 states of Sudan. The fighting has destroyed critical infrastructure — hospitals, schools, water systems — and decimated the humanitarian architecture that millions depended on. By December 2025, 8.3 million people were internally displaced across Sudan, with an additional 2 million fleeing to neighbouring countries.
The conflict zones have shifted over time, expanding from Khartoum and the Darfur states into previously stable regions including Aj Jazirah, Sennar, and Blue Nile. In October 2025, after 540 days of siege, El Fasher in North Darfur fell to RSF forces, with reports of mass atrocities and a catastrophic humanitarian crisis following. The pattern is grimly consistent: wherever fighting intensifies, civilian suffering — and GBV in particular — escalates dramatically.
GBV: A Weapon of War
The scale and severity of gender-based violence in Sudan is staggering. The number of people in need of GBV services has doubled since the conflict began, rising from 3.1 million before April 2023 to 6.9 million by end of 2024, and the population at risk has reached 12.1 million — an 80 percent increase from the previous year. There is mounting evidence that rape is being used deliberately and systematically as a weapon of war, particularly by RSF forces in areas under their control in Khartoum, Bahri, and Omdurman.
The forms of violence reported across Sudan are wide-ranging and deeply interlinked with the dynamics of conflict and displacement:
Conflict-Related Sexual Violence
Rape, gang rape, and sexual assault used as weapons of war, particularly during military operations and the takeover of towns and IDP camps.
Forced & Child Marriage
Economic desperation and displacement are driving a surge in early and forced marriages, used as a coping mechanism by families in crisis.
Sexual Exploitation & Survival Sex
Women and girls are coerced into sex in exchange for food, shelter, or safe passage — particularly at checkpoints and distribution sites.
Intimate Partner Violence
Domestic violence has intensified due to economic stress, displacement trauma, and the breakdown of community support structures.
Critically, only 3 percent of humanitarian funding reaches women-led organisations directly, and specialised GBV services — case management, psychosocial support, legal aid, and referral mechanisms — remain severely underfunded and geographically patchy. Between January and July 2025, UNFPA reached 270,000 people through 75 women- and girl-friendly safe spaces and 90 community protection networks, but this represents a fraction of those in need.
Displacement & GBV Data: The Evidence
The interactive dashboard below draws on UNHCR operational data (December 2025) and the 2025 Humanitarian Needs Overview (HNO) dataset to visualise the scale of displacement across Sudan’s 18 states, the severity of GBV needs in Blue Nile State, and the critical gap between humanitarian presence and GBV-specific programming.
Internal Displacement by State
Sudan: IDP Distribution by State
Blue Nile State: GBV Severity & People in Need
GBV People in Need by Locality
GBV Severity Ratings (HNO 2025)
| Locality | GBV Severity | Protection | Child Protection | Final Severity | GBV PiN |
|---|---|---|---|---|---|
| Ed Damazine | 4 — Extreme | 4 | 3 | 3 | 138,405 |
| Ar Rusayris | 4 — Extreme | 3 | 4 | 3 | 59,917 |
| Bau | 4 — Extreme | 3 | 3 | 4 | 44,427 |
| Geisan | 4 — Extreme | 4 | 4 | 3 | 37,256 |
| At Tadamon | 4 — Extreme | 4 | 4 | 4 | 27,058 |
| Al Kurmuk | 4 — Extreme | 4 | 4 | 4 | 23,557 |
| Wad Al Mahi | 3 — Severe | 3 | 3 | 3 | 9,328 |
Blue Nile Localities: GBV Severity Map
Humanitarian Service Coverage in Blue Nile State
Organisations by Sector
GBV Actors by Locality
| Locality | GBV Actors | Organisations | GBV PiN |
|---|---|---|---|
| Ar Rusayris | 5 | CDF, HANDs, IMC, IRC, RI | 59,917 |
| Ed Damazine | 4 | HANDs, IMC, RI, SFPA | 138,405 |
| Bau | 2 | IMC, IRC | 44,427 |
| Wad Al Mahi | 2 | IMC, IRC | 9,328 |
| Geisan | 1 | RI | 37,256 |
| Al Kurmuk | 0 | — None — | 23,557 |
| At Tadamon | 0 | — None — | 27,058 |
Blue Nile State: Ground Zero
Blue Nile State, in Sudan’s southeast bordering Ethiopia and South Sudan, has become a contested battleground involving three armed factions: the SAF, RSF, and SPLM-N (al-Hilu) forces. Fighting in Kurmuk County escalated significantly in early 2026, displacing tens of thousands more people into already overcrowded host communities and informal settlements.
The 2025 Humanitarian Needs Overview dataset paints a stark picture: GBV severity is rated at level 4 (extreme) in six of seven localities, with approximately 339,948 people in need of GBV services. Ed Damazine, the state capital, alone accounts for over 138,000 GBV-affected individuals — more than the total GBV caseload of many entire states.
The Service Gap: 51 Organisations, Only 6 for GBV
The 4Ws (Who does What, Where, and When) dataset for Blue Nile State reveals a fundamental mismatch between humanitarian presence and GBV service delivery. While 51 organisations operate across the state — covering water, food, health, nutrition, and shelter — only 6 are registered GBV actors: IMC, IRC, RI, HANDs, CDF, and SFPA. And their coverage is deeply uneven.
Ar Rusayris — Best covered
Five GBV actors (CDF, HANDs, IMC, IRC, RI) — the only locality approaching adequate coverage for its 59,917 GBV PiN.
Ed Damazine — Largest need, moderate coverage
Four GBV actors (HANDs, IMC, RI, SFPA) for the state’s highest GBV caseload of 138,405 people. The ratio of need to capacity here is alarming.
Geisan — Critically underserved
A single GBV actor (RI) serving 37,256 people in need. One organisation cannot provide the multi-sectoral GBV response this caseload demands.
Al Kurmuk & At Tadamon — Complete absence
Zero GBV actors despite a combined 50,615 people in need and extreme severity ratings (level 4). These are also the localities nearest the active front lines and South Sudan border crossings.
This gap between overall humanitarian presence and GBV-specific programming is not unique to Blue Nile — it reflects a systemic pattern across Sudan where GBV is consistently among the least funded and least resourced sectors of the humanitarian response. Yet the evidence is clear: where GBV services are absent, survivors have nowhere to turn, cases go unreported, and the cycle of violence deepens.
Bridging the Gap
In response to the critical service gaps documented above, efforts are now underway to conduct a comprehensive GBV service mapping and develop a functional GBV referral pathway and GBV pocket guide for Blue Nile State, with a focus on Kurmuk County and Yabus Payam. This work employs a participatory, survivor-centred, mixed-methods approach grounded in IASC GBV Guidelines, GBV Minimum Standards, and GBV Area of Responsibility (AoR) frameworks.
The initiative directly addresses the documented gaps: understanding why 51 organisations operate in Blue Nile yet only 6 deliver GBV services, what cross-sectoral actors can do to integrate GBV risk mitigation, and how functional referral pathways can connect survivors to the help they need — particularly in Al Kurmuk and At Tadamon where no GBV actors currently operate.
Conclusion
Sudan’s GBV crisis is not a secondary consequence of conflict — it is a defining feature of it. The systematic use of sexual violence as a weapon of war, the 288 percent surge in demand for services, and the stark absence of GBV actors in some of the most affected localities all point to a crisis that demands urgent, evidence-based action.
The data from Blue Nile State illustrates both the severity of the challenge and the pathway forward. With 339,948 people in need of GBV services across seven localities, with six rated at extreme severity, and with two localities lacking any GBV presence whatsoever, the gap between need and response has never been more clearly documented. Ongoing service mapping and referral pathway development represent a concrete step toward closing that gap — building the evidence base, coordination tools, and referral mechanisms that survivors and service providers urgently need.
As Sudan enters its third year of conflict, the humanitarian community must recognise that GBV programming is not optional — it is a core component of effective humanitarian response. Every service mapped, every referral pathway strengthened, and every pocket guide placed in the hands of a frontline worker moves us closer to a response that truly serves those most affected by this crisis.